Rising Together: The Parallel Growth of Obesity and Mental Health Conditions

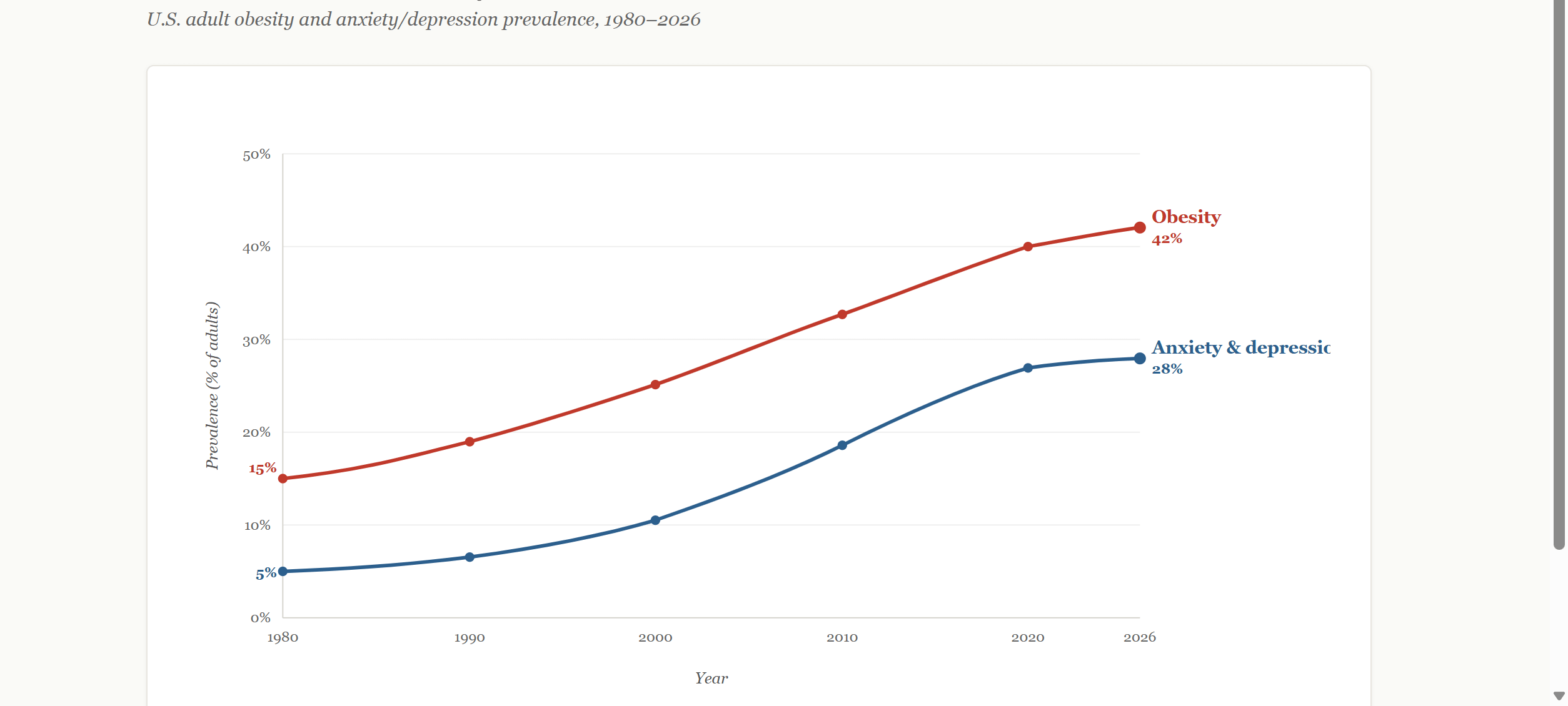
If you laid two graphs on top of each other, one tracking the rise of obesity rates and the other tracking the rise of depression and anxiety, you would see something unsettling…the lines move together. At some point, a reasonable person has to stop and ask the obvious question, is it just a coincidence? For a long time, public health treated these trends as if they were. Obesity was a problem of diet, activity, and environment while depression and anxiety were problems of brain chemistry, life circumstances, and stress.
Coincidences of this scale should not be ignored, and may suggest a single system under strain, with each condition feeding into the other. Once you can see it that way, a lot of the confusion in how we treat these conditions starts to make sense, and a lot of the frustration patients feel starts to make sense too.
A woman in her forties develops depression after a difficult stretch at work. She sleeps poorly, stops exercising, starts eating for comfort, and her doctor prescribes an antidepressant that contributes to gradual weight gain. Two years later, she is carrying an extra thirty pounds, her inflammatory markers have risen, her joints ache, and she feels judged every time she walks into a medical office. The weight is now making her depression worse and the depression is now making the weight harder to address. Which one do you treat first?
Traumatic experiences, difficult childhoods, and major life upheavals can significantly contribute to obesity. When people endure chronic stress or emotional pain, the body produces elevated levels of cortisol, a hormone that increases appetite and promotes fat storage, particularly around the abdomen. Childhood adversity, such as abuse, neglect, or household instability, can disrupt the development of healthy emotional regulation skills, leaving people more likely to rely on food to serve as a protective response, whether by creating a physical buffer against unwanted attention or simply by providing one of the few accessible sources of pleasure in a painful environment. Major life transitions such as divorce can disrupt routines, increase stress, and reduce time or energy for self-care, all of which can tip the balance toward weight gain. Many individuals turn to food as a coping mechanism, using eating to soothe emotional distress, fill feelings of emptiness, or experience a fleeting sense of comfort and control during periods when life feels chaotic. Recognizing these connections is important because it reframes obesity not simply as a failure of willpower but often as a symptom of deeper emotional wounds that deserve compassionate attention and, frequently, professional support.
Depression and anxiety don’t just affect mood, they alter the body in ways that make weight gain more likely. Sleep is often one of the first systems disrupted, and poor sleep throws off key hormones like leptin and insulin, both of which regulate appetite and mood. As these signals fall out of balance, cravings intensify, particularly for high-calorie foods. At the same time, depression blunts motivation, and makes regular physical activity harder to sustain, reinforcing a more sedentary pattern over time.
Medication complicates the picture further. Many commonly prescribed antidepressants, antipsychotics, and mood stabilizers carry weight gain as a known side effect. A person seeking treatment for their mental health can find themselves, a year or two later, twenty or forty pounds heavier, with a new medical problem layered on top of the one they came in to treat.
Looking at it in reverse, individuals with obesity carry roughly a 32% higher risk of developing depression. The risk is often stronger in women, where higher adiposity is more tightly linked to lower quality of life, mood disorders, and anxiety. Then there is the social layer, adults carrying extra weight are routinely dismissed, overlooked in hiring, judged in social situations, and told, implicitly or explicitly, that their bodies represent a personal failing. That kind of chronic, cumulative rejection corrodes self-worth, feeds anxiety, and deepens depression.
Obesity produces chronic low-grade inflammation throughout the body, and a growing body of research implicates that inflammation directly in the development of depressive symptoms. Elevated CRP, IL-6, and TNF-alpha, all common in obesity, are also increasingly recognized as markers and drivers of depression. The HPA axis, the body’s central stress response system, is dysregulated in both conditions, making it one of the most well understood shared biological pathways between them.
The suicide data in this space also deserves closer attention. Depression and anxiety are among the most significant modifiable risk factors for suicide, and over the past two decades, adult suicide rates in the United States have risen sharply, with particularly concerning increases among younger populations. These trends overlap with the same period in which both obesity and mental health conditions have increased. Because obesity is associated with a higher risk of developing depression and anxiety, it may also play a role upstream of suicide risk, a possibility that warrants further study. The connection is not direct or universal, but the pathways are meaningful, with biological factors like chronic inflammation and hormonal disruption, along with psychological strain and social pressures such as stigma and isolation, compounding vulnerability over time.
Mental health screening should be a routine part of care for adults being treated for obesity yet many clinical conversations about obesity still center on calories, physical activity, and, more recently, GLP-1 medications. Conversations about depression, by contrast, tend to focus on therapy, medication, and lifestyle change. These discussions take place in different rooms, led by different specialists, and are often separated even at the level of insurance. The result is fragmented care, handled in sequence rather than as a whole, which simply recreates the same trend seen in the data: two curves rising in tandem, with millions of people caught between them.
The pattern of obesity and mental health isn’t subtle, and it isn’t short-lived. It’s been building in parallel, in the data and in real lives, for decades. Turning a blind eye to that connection doesn’t make it disappear, it just ensures the trajectory continues.